


Bonne St Jean-Baptiste 2025
Like Passover, a lot can happen in eight days

I should note that I couldn’t think of a creative name to this post, and as yesterday, when I started this post, was the feast day of Saint John the Baptist (who is the patron saint of the province of Quebec, as well as of the Spanish province of Catalonia and the US territory of Puerto Rico), and as I saw the following graphic on my feed from Statistics Canada…

I decided to name today’s post for it. The Statistics Canada Facebook post, linked to an article on the Statistics Canada website that discusses francophone Canada, its distribution, population, etc. It’s a quick read.
Even though I didn’t note it in my last Substack post (Cultural Collisions And Communal Costs, given it was a discussion of Anne Fadiman’s book The Spirit Catches You and You Fall Down), nor the one previous to that (It's Not Just The Food - A Presentation, given that was a class presentation), as both of those were specific to their content only, but there were three big events last week, two being macroscale: First, on 14 June, was the 250th anniversary of the founding of the United States Army (“This We’ll Defend”), and, second, on 16 June was the 250th anniversary of the founding of the US Army Corps of Engineers (“Essayons”), and one a lot more microscale - which is the fact that on 17 June, I was notified by the University of Washington that I had been admitted to do a post-baccalaureate degree in microbiology. I will discuss this a bit further on in this post, but before I do, let me reflect a little on my last five weeks of public health courses at UVM.
Numero Uno - Five Weeks of UVM Public Health
As of last Sunday at roughly 23h30 pacific time - I finished my last assignment I had to complete for PH 6010, which meant I was done with all of my coursework for my two public health courses.
The courses described, are as follows:
PH 6010 - Public Health & Health Policy
This course provided a broad foundation in public health principles, policies, and population-level health challenges. From the start, it emphasised that public health is not simply clinical care - it is prevention, systems thinking, and addressing the social and structural factors that shape health outcomes.
We explored how policies - both effective and lacking - impact major public health issues. The opioid epidemic illustrated how stigma, underinvestment, and fragmented policies perpetuate preventable deaths, while tobacco control efforts demonstrated how litigation, regulation, and public campaigns can reduce harm, though debates over e-cigarettes and harm reduction continue.
It was for this class that I created what became my previous Substack post - Public Health Through the Lens of Systems Engineering.
Mental health was framed as a critical public health issue, with COVID-19 further exposing the system’s gaps. We examined how stigma, lack of access, and structural inequities disproportionately affect youth, rural populations, and marginalised groups.
Chronic disease prevention showed how policies targeting nutrition, like sugar-sweetened beverage taxes, intersect with equity, economics, and health behaviour change. The module on firearm injury prevention reinforced how health, culture, and politics collide - with rural, urban, and demographic patterns revealing stark disparities, including among veterans.
Across these topics, a consistent theme emerged: public health requires coordinated policy, systems reform, and an understanding of social determinants—not just medical care. Applying a public health lens to issues like veterans’ disability policy reinforced how health outcomes are shaped by employment, access to care, and systemic design.
In sum, this class taught that public health is complex, political, and essential to building healthier, more equitable communities.
PH 6060 - Social & Behavioural Public Health
This course provided a comprehensive introduction to the theories, models, and practical strategies that guide behaviour change and health promotion efforts at individual, community, and population levels. The course emphasised that health behaviours do not occur in isolation but are shaped by complex ecological, cultural, and structural factors.
Early modules introduced foundational health behaviour theories, including the Health Belief Model, Social Cognitive Theory, and the Ecological Model. These frameworks provided a lens for understanding how knowledge, beliefs, environment, and social norms influence health-related choices. The course consistently underscored the role of structural bias, social inequities, and systemic racism in undermining health equity - drawing connections to real-world public health challenges such as obesity, addiction, and chronic disease management.
A key thread throughout the course was the importance of cultural humility and tailoring interventions to the lived experiences of target populations. Through analysis of case studies - including the Hmong refugee experience in The Spirit Catches You and You Fall Down - students explored how health systems can either perpetuate inequity or foster trust through respectful, community-engaged approaches.
Later modules focused on communication and implementation science, examining how social marketing, fear appeals, social media, and behavioural economics can be leveraged to promote positive health behaviours. Students developed practical skills in creating health communication materials with attention to literacy, cultural relevance, and platform-specific strategies.
The course concluded by reinforcing that sustainable health behaviour change requires multi-level interventions, structural supports, and continuous engagement with affected communities.
In sum, PH 6060 equipped students with both the theoretical foundation and applied tools to design public health initiatives that are effective, equitable, and grounded in respect for diversity and complexity.
=//=
Of the two, PH 6060 was a lot more personally resonant, and the one I enjoyed more, however both of these courses have been useful for expanding my knowledge and skill set.
Trying to crank out all of the work by last Sunday was a bit rough though, since it required me compressing two weeks work of work for both classes in just a few days, but since I didn’t want the UVM course material hanging over on me during my first week at UW this summer. I felt a bit like a drained husk by Sunday night, but at least I was able to get it done.
Numero Dos - UW and the Remainder of my Pre-Med Prep
Given the fact that I knew I’d be returning to Seattle to help take care of my father, and do the remainder of my UVM work from home, this also meant that I couldn’t use my UVM biomedical engineering masters to do what I originally intended for it, which was to use it to shoehorn in all of the pre-med pre-reqs, so that I’d have to do those at my primary undergraduate alma mater - the University of Washington - back home in Seattle.
As I have discussed previously - in my UVM first anniversary Substack post - I knew at a minimum, at UW, I’d have to cover third quarter intro biology (Biology 220), first quarter organic chemistry (Chem 237), as well as the two quarter biochemistry series, BIOC 405 and BIOC 406, would bring me up to minimum qualifying standards for med school admissions.
However, as I’m looking to do all that I reasonably can to prepare myself for medical school, and once I figured out that trying to arrange visiting graduate student status at UW was not a realistic possibility, I admittedly started looking at applying to be a post-baccalaureate student at UW, given in no small part my concern that UW school of medicine, at least for their first round of admissions, has a very formulaic system for admissions, one that my status as a career changer, especially with my (for med school purposes) non-traditional CV - even for career changers - given my age (I am over 40 now), educational and career background (not many people who apply for med school have grad degrees at all, and most of those that do have a single masters, and either with a Masters in Public Health or the Masters in Medical Sciences that many applicants who need CV bolstering enrol in - not an engineering masters, much less two of them, or in my case, 2.5 of them since I’m now coursework complete in my third masters in my third different engineering discipline), status as a veteran (and a disabled veteran at that), etc.1
So, I applied as a post-bac student to take another bachelors degree in microbiology, and on 17 June, after an initial rejection and filing an appeal, my admission as a UW post-bac for microbiology was accepted.
For anyone who wants to ask about if this means I’m giving up my UVM biomedical engineering masters - no I am not. I did the two public health courses to make sure that I was coursework complete for that degree, so that I would only have to do the remainder of my thesis work.
So, the initial plan for me for my microbiology post-bac, for my courses, are as follows:
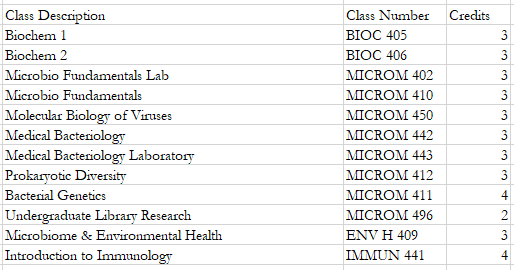
Since the two quarter biochem series is a degree requirement for the BSc in microbiology, that will remain the same for me. Everything else is a core or elective Microbiology degree requirement, which maps to the distribution requirements, required number of lab courses for the degree, etc.
So, when completed, this would, on top of everything else I’ve done, bring me up to parity to traditionally prepared aspiring med students with life sciences degrees. This will also make me more able to compete for jobs applying to work in wet labs, at biotech firms, etc., so if I have to stretch out my med school application process into a another year cycle, I’ll be able to find relevant work towards my med school application in the mean time.
Since all of this stuff happened in an eight day window, it felt very Passover-esque to me, and as happy as I am to be here now, I was also pretty spent come yesterday, and admittedly as well today, given all of the admin things I have to get done to do my post-bac in microbiology, including a lot of admin stuff, a non-trivial portion of which stems from the fact that, because I also did the bulk of my undergrad at UW, and took a degree from here in 2009, there are some artifacts in various systems that stem from my previous period as a matriculated student here, but those I am working through as well, which is part of why I feel so spent right now.
On that note, that’s the full lid on this Wednesday, 25 June 2025.
This concern is a very personal one for me, given that, of the universities I applied to out of secondary school, UW was the only one to reject me (even though most of the other universities that I got into had higher admissions standards at that time than UW) & I definitely didn’t want to go through that experience again when applying for med school.